2038
Views & Citations1038
Likes & Shares
Darier’s disease (DD) or Keratosis follicularis is a
rare dominantly inherited genodermatosis characterized clinically by presence
of multiple pruritic discrete scaly and keratotic papules in seborrheic areas
of the body with characteristic nail involvement and mucosal lesions.
Histologically focal areas of acantholysis in the suprabasal layer of epidermis,
lacunae within the epidermis and dyskeratosis are seen. Segmental forms of
Darier's disease are classified into two clinical subtypes: type 1 with
distinct lesions on a background of normal appearing skin and type 2 with
well-defined areas of Darier's disease occurring on a background of less severe
non-mosaic phenotype. Although there are several clinical variants of Darier's
disease, few cases of segmental Darier's disease have been described in the
literature. We describe a 31 year old lady with type 2 segmental Dariers
disease. This unique clinical variant of Darier's disease has been described
very rarely.
Keywords:
Darier’s disease, Genodermatoses, Acantholysis, Dyskeratosis, Type 2 segmental
INTRODUCTION
Darier’s disease is a rare autosomal dominant
genodermatosis, initially described by Prince Marrow in 1886 and later by
Darier and White in 1889. It has high penetrance, variable expressivity and
worldwide distribution [1,2]. It is caused by a defect in ATP2A2 gene located
on 12q23-23 chromosome [3]. The onset of DD generally occurs during the first
two decades of life, although onset as late as the fourth decade is not
uncommon [4]. It mainly presents over the seborrhoeic areas as multiple
brownish and pruritic papules along with palmoplantar pits, nail dystrophies
(V-shaped nicking and ridging), hyperkeratotic papules on the dorsal aspects of
the hands and feet and cobblestone papules may be seen on oral mucosa [1,4].
Histopathologically characterized by focal suprabasilar acantholysis and
dyskeratotic keratinocytes known as corps ronds and grains in the stratum
spinosum and corneum, respectively [2,3].
CASE REPORT
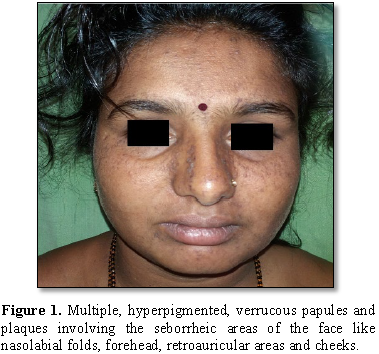
A 31 year old lady presented with multiple verrucous lesions on face, trunk, upper and lower limb since childhood. There was history of photosensitivity. The lesions aggravated on sun exposure. Family history was non-contributory. Cutaneous examination revealed multiple, hyper pigmented, verrucous papules and plaques involving the seborrheic areas of the face like nasolabial folds, forehead, retroauricular areas and cheeks (Figure 1).Lesions were also present on the neck and right supraclavicular area (Figure 2).
Figure 2. Multiple, hyperpigmented, verrucous papules
and plaques on the neck and right supraclavicular area.Few lesions
were distributed linearly on right forearm and dorsum of right foot extending
to the leg (Figure 3).Multiple
guttate, hypopigmented macules were seen over the arms, abdomen and chest (Figures 4 and 5).
Figure 6. Showing hyperkeratosis,
acanthosis, hypergranulosis, corps rounds in granular layer. Superficial dermis
shows mild perivascular lymphocytic infiltrates.
The diagnosis of type-2 segmental Darier’s
disease was made based on clinical and histopathological examination. The
patient was treated with oral Isotretinoin 20 mg OD, topical tretinoin 0.05%
cream, emollients and a broad spectrum sunscreen. One month later, marked
improvement was noticed in the form of reduced photosensitivity and flattening
of lesions over the nasolabial fold and on legs (Figure 7).
DISCUSSION
DD was independently reported by Darier and
White in 1889 [2]. Its pathogenesis has been linked to mutations involving the
ATP2A2 gene that codes for sarco/endoplasmic reticulum calcium ATPase isoform
2, a pump that transports calcium (Ca2+) from cytosol to lumen of
the endoplasmic reticulum, thus hampering the intracellular Ca2+
signaling and keratinocyte intercellular adhesion and differentiation [5]. The
clinical findings in Darier’s disease include keratotic, crusted red-brownish
papules distributed over the seborrheic areas such as trunk, scalp margins,
face and lateral aspects of the face. The papules generally coalesce to form
large verrucous plaques. Nearly half of the patients have flat, shiny warty
papules on the dorsal aspect of the hands. Painless whitish papules may be
observed in oral mucosa in 15% of patients [3]. Variants of Darier's disease,
including linear, bullous and generalized hypertrophic types, have been
reported. Although patients with the disorder are not systemically ill, both
mild and severe disease may be disfiguring, with profound effects on
self-image. Pruritus occurs in many cases and is often severe. Secondary
bacterial contamination of the skin is not uncommon, with pyoderma and a
refractory malodor often resulting [6].
After reports of unilateral or zosteriform
patterns in patients with Darier’s disease, the synonyms acantholytic
dyskeratotic epidermal nevi, segmental Darier’s disease, linear Darier’s
disease and localized Darier’s disease were started to be used for describing
mainly the same localized clinical condition observed in Darier’s disease.
About 10% of patients with Darier’s disease are estimated to have linear or
zosteriform pattern, localized on one-half of the body and linear Darier’s
disease is accepted as a mosaic form of Darier’s disease [3]. Two patterns of
segmental DD are recognised namely type 1 and type 2 segmental Dariers disease.
In type 1 pattern, lesions follow Blaschko’s lines unilaterally, whereas a type
2 disease demonstrates focal areas of increased severity in patients with
generalized DD. In our patient, the verrucous lesions were predominantly on the
right side of the body. Lesions in the supraclavicular area were distributed in
zosteriform pattern and those on the right leg were in arranged linearly. Also,
guttate hypopigmented macules were found on the left forearm, abdomen and back.
Localized DD is considered a genetic mosaic
of generalized DD resulting from a post-zygotic somatic mutation in early
embryogenesis. The zosteriform pattern described in localized DD would actually
exhibit a Blaschkoid rather than a dermatomal distribution [5].
Abnormal keratinocyte-keratinocyte adhesions
and aberrant epidermal keratinisation are histological features of DD.
Histology shows dyskeratosis in spinous layer (corps rounds) and stratum
corneum (grains), suprabasal acantholysis and clefts (lacunae). The underlying
dermal papillae, covered by a single layer of epithelium (stratum basale),
project into these clefts and form villus like structures. A large keratin
plug, often showing focal parakeratosis, overlies each lesion. Hyperkeratosis
is common [4,6]. Electron microscopy reveals loss of desmosomes, breakdown of
desmosomes keratin intermediate filament attachment and perinuclear aggregates
of keratin intermediate filaments. The differential diagnosis includes acne
vulgaris, seborrheic dermatitis, acanthosis nigricans, confluent reticulate
papillomatosis, prurigo pigmentosa and reticulate erythematomucinous syndrome.
In acanthosis nigricans lesions are more pigmented. In confluent reticulate
papilomatosis the lesions are flat and confined to upper trunk. The harshness
of papules on palpation helps to distinguish it from visually similar
conditions like prurigo pigmentosa and reticulate erythematomucinous syndrome.
Histologically the disease needs differentiation from benign familial
pemphigus, Grover’s disease and pemphigus vulgaris. Immunofluroscence of skin
biopsy differentiate different acantholytic disorders [2].
The basic principles in the control of
Dariers disease is avoidance of ultraviolet (UV) light, sweating and
maintainence of personal hygiene [4]. Systemic retinoids have been the most
effective treatment modality for generalised forms, but the side-effect profile
limits their use [1]. Treatment options for segmental DD mainly include topical
therapies because of localized involvement. Avoiding precipitating factors such
as sunlight and heat may improve the symptoms. Emollient containing urea or
lactic acid helps in reducing crusting and irritation. Topical retinoids
improve the lesions by reducing hyperkeratosis. Successful treatment of
segmental DD using ablative fractional laser resurfacing has been reported [5].
Patient should be informed about the
complications and the care required. The emotional status should be evaluated
[9]. Regardless of clinical severity and treatment options, the patient should
receive genetic counseling with information on inherited condition and risk of
transferring to offspring.
1. Bakar O, Durmaz EO, Sezer E, Çetin
ED (2015) Type 1 segmental Darier's disease: Report of two cases with favorable
response to topical retinoids. Hong Kong J Dermatol Venereol 23: 71-75.
2. Mahboob A, Yaqub F, Shahzad Z,
Afzaal M, Hanif M, et al. (2010) Classical presentation of Darier’s disease: A
rare disorder of keratinisation - Case report. J Ayub Med Coll Abbottabad 22:
230-233.
3. Dogan S, Karaduman A, Erkin G,
Gokoz O (2011) Effective treatment of linear Darier’s disease with topical
retinoids: Case report and review of the literature. Acta Dermatovenerol Croat
19: 206-211.
4. Bhat RM, Ullal KR, Pinto AC,
Sukumar D (2010) Darier-White disease in siblings responding to isotretinoin.
Indian Dermatol Online J 1: 18-20.
5. Palanisamy A, Kandasamy S, Vadivel
S, Kothandapany S (2015) Type one segmental Darier’s disease. Indian J Dermatopathol
Diagn Dermatol 2: 34-36.
6. Del rosso JQ, Horowitz DC (1986)
Treatment of Darier's disease with isotretinoin: Report of a case. J AOA 86:
634-638.






QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Journal of Pathology and Toxicology Research
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)


